
Brain imaging studies support the idea that the sympathetic nervous system (SNS) is hyperactive in fibromyalgia. To understand the brain evidence we first need to explore how the brain normally regulates the SNS, and then look at the ways this go wrong in fibromyalgia. My aim here is to share information about the SNS in the fibromyalgia brain in a way is accurate, clear, and accessible to everyone.
Neuroscience is intricate and complex. Writing these posts required me to dig deep back into my medical school textbooks! Brain science is also rapidly evolving as we find newer and better ways to study the brain. Most generalist health care providers, if they are honest with themselves, are probably a bit rusty on some of the more intricate details of brain function.
The pistachio running the show
So let's start with a refresher about the role of the SNS. It operates one side of the autonomic nervous system (ANS), which I like to call our "autopilot" nervous system because it regulates most bodily housekeeping functions. In a simplistic way we can think of the autopilot nervous system primarily as being run by hypothalamus, a deep brain structure that is the size of a pistachio. It is actually a "committee" of different brain areas that work together to manage this large and complex nerve network.
Let's ease our way in and start looking how the brain normally controls ANS function, then we will explore where that is misfiring in fibromyalgia. There are a few ways scientists can measure brain activity. The first is with specialized brain scans called functional MRIs, that measure blood and oxygen levels in the brain to detect activity. The areas lit up in the functional MRI brain imaging in figure 1 consists of the many players on the team controlling the ANS. This leadership committee is often called the Central Autonomic Network. Several different parts of the brain manage this complex network of nerves including parts of the prefrontal cortex, limbic system, brain stem and the hypothalamus, which acts as the captain of this motley crew.
How does a functional MRI work?
The BOLD signal (Blood Oxygen-Level Dependent signal) is the fundamental signal measured in fMRI (functional Magnetic Resonance Imaging) that shows brain activity by detecting changes in blood oxygenation, reflecting neural activity indirectly. When neurons fire, they use oxygen, causing a temporary rise in deoxygenated hemoglobin, which slightly weakens the MRI signal, but this is followed by a disproportionate increase in blood flow that brings in more oxygenated blood, ultimately boosting the signal. This hemodynamic response (the BOLD signal's rise and fall) allows scientists to map which brain areas are active during tasks, even though it's an indirect, delayed, and complex measure.
Functional MRIs of the brain can show which parts of the brain are active at any one time, but it's a static image, like a group picture of a sports team. It only shows us who is present on picture day! Get more useful information about how a team works by seeing how they play the game together. This type of MRI can also be used to look for connections (functional pathways) between different parts of the brain.
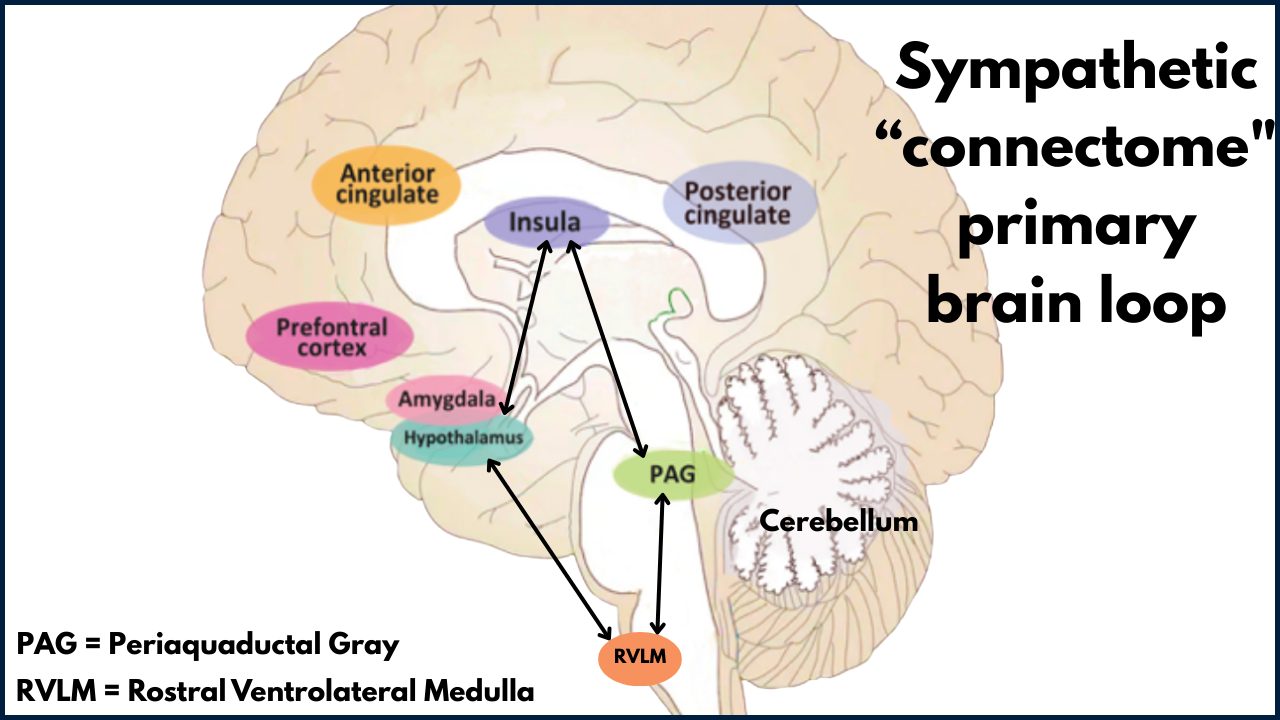
Researchers have identified four key areas of the brain that regulate SNS and have especially strong connections to each other. The insula, the hypothalamus and areas in the brain stem (PAG and RVLM) form a brain circuit, or loop, that runs the SNS show. Scientists have termed this brain circuit the “human sympathetic connectome”.
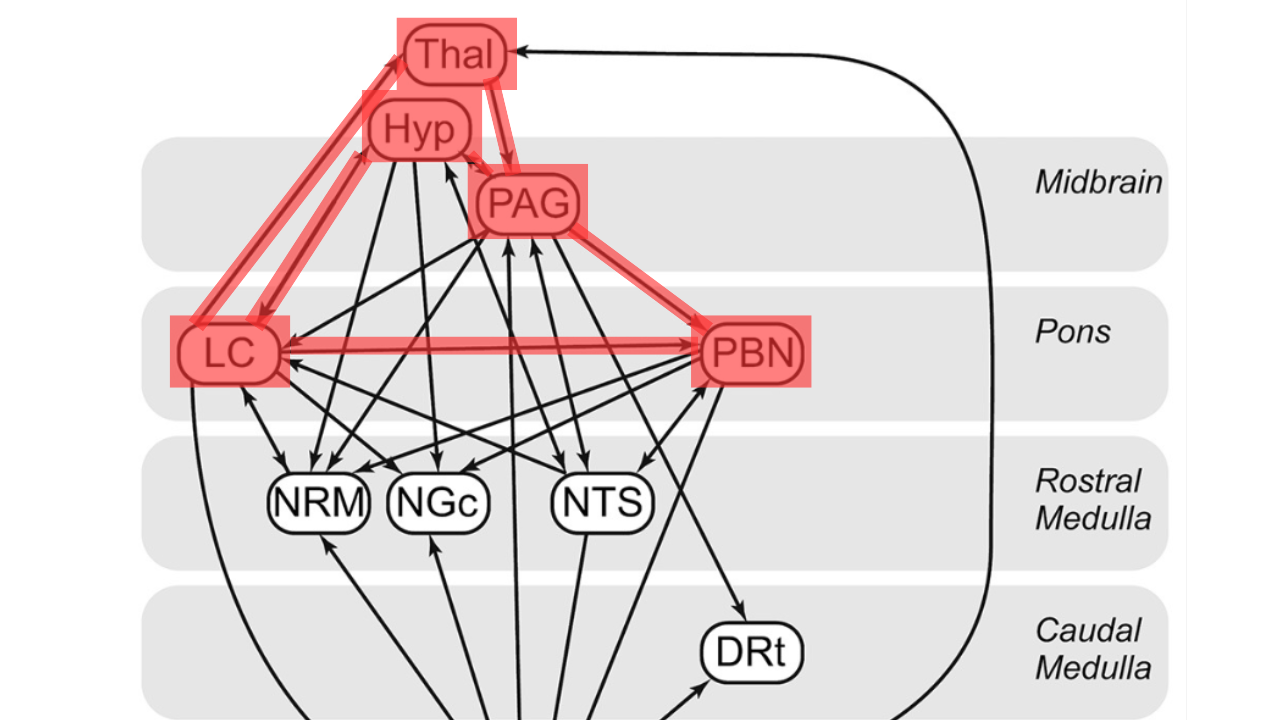
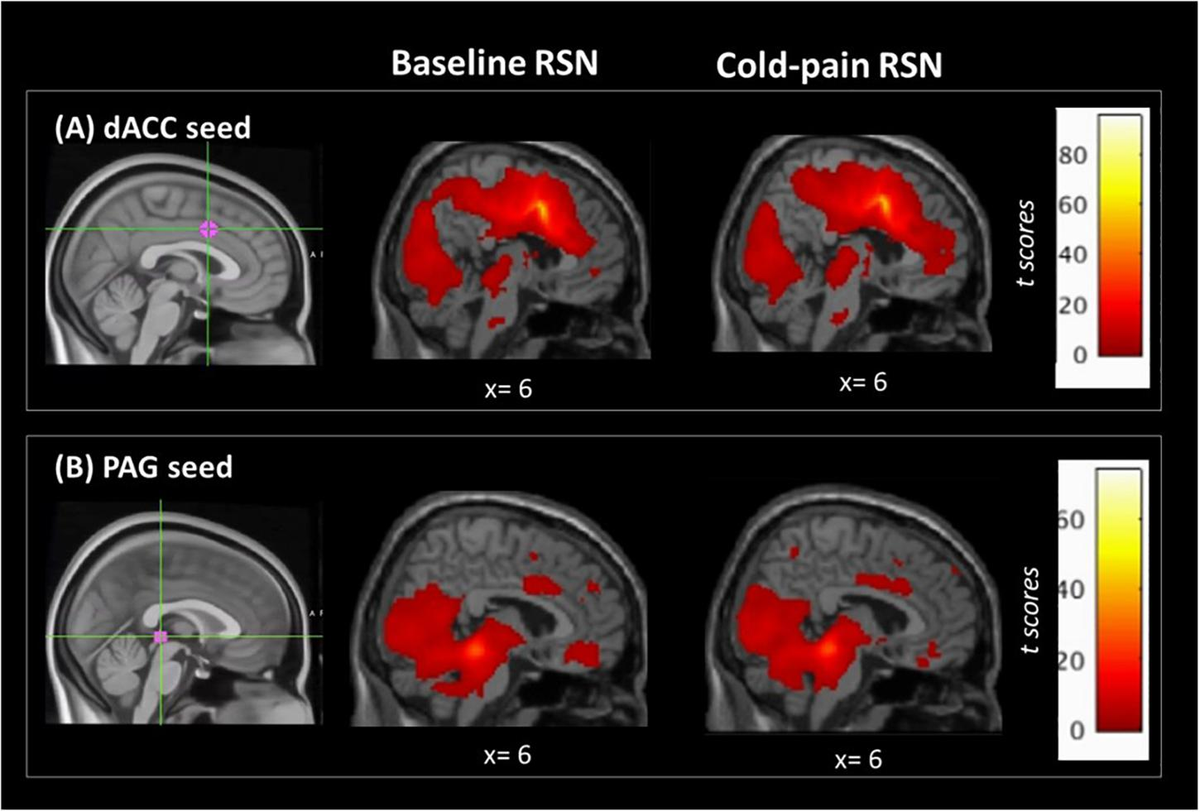
Several of these key areas of SNS control brain circuit show abnormal activity in fibromyalgia, including the insula, hypothalamus and PAG. In addition to this core leadership team there are other parts of the brain that play key roles in managing the SNS, and they aren't working correctly in fibromyalgia either! Imaging studies also reveal higher levels of activity and connections between other brain regions that play a role in managing the SNS including the thalamus, locus coeruleus (LC), and parabrachial nuclei (PBN) as shown below in figure 3.
One study looked at how the fibromyalgia brain responded to painful stimuli, and found increased connectivity between the posterior cingulate cortex (PCC) and the thalamus compared to heathy brains. The PCC is part of the Central Autonomic Network and the thalamus is the main pain relay station of brain. This enhanced connectivity may be one way the brain "pays more attention" to painful stimuli, we may actually be seeing part of the actual brain mechanism that causes hyperalgesia (amplification of pain signals) in fibromyalgia. Another study found that levels of increased connectivity between the PAG and other brainstem regions involved in ANS signaling varied with a participant’s pain score, meaning stronger connections were seen in those with higher fibromyalgia pain levels.
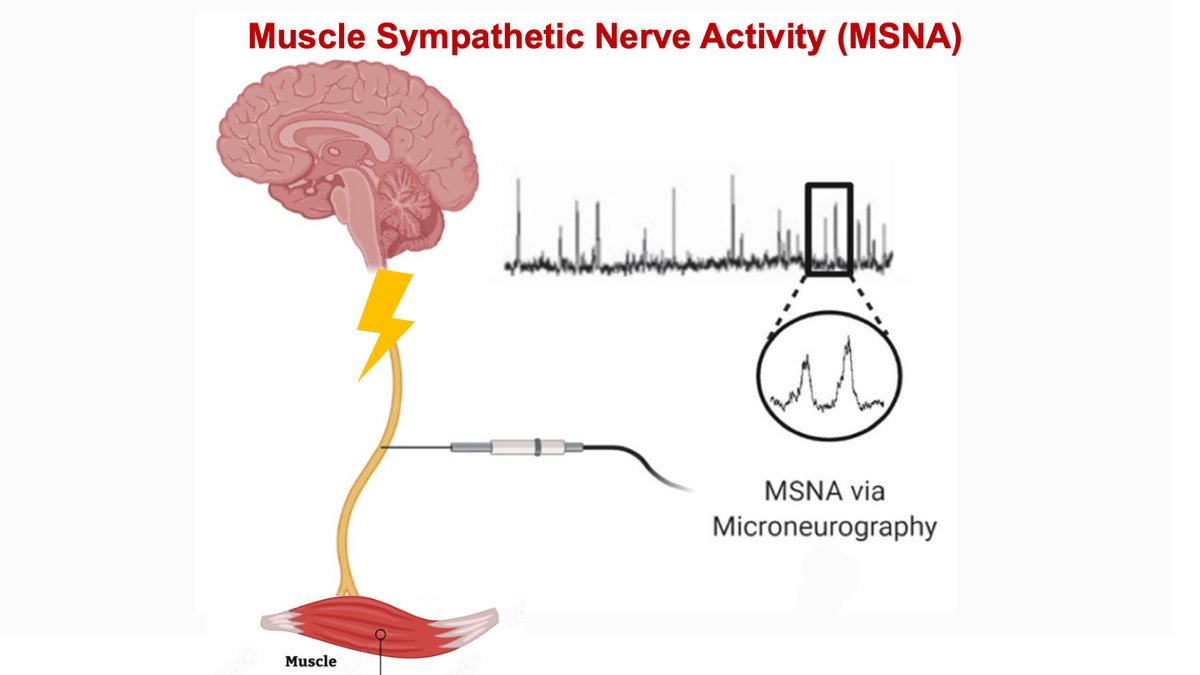
Another way we can find out which areas of the brain regulate what body functions is by electrically stimulating different regions and seeing what changes occur in the body. This is more of a "poke it with a stick and see what happens " approach. For example, electrical stimulation of the PAG region via deep brain stimulation triggers the brain to send stronger electrical pulses down the sympathetic nerves to the muscles. Because we see the same pattern of elevated muscle sympathetic nerve activity fibromyalgia muscles, working backwards we can assume this stems from increased activity in this part of the brain in fibromyalgia.
The plot thickens
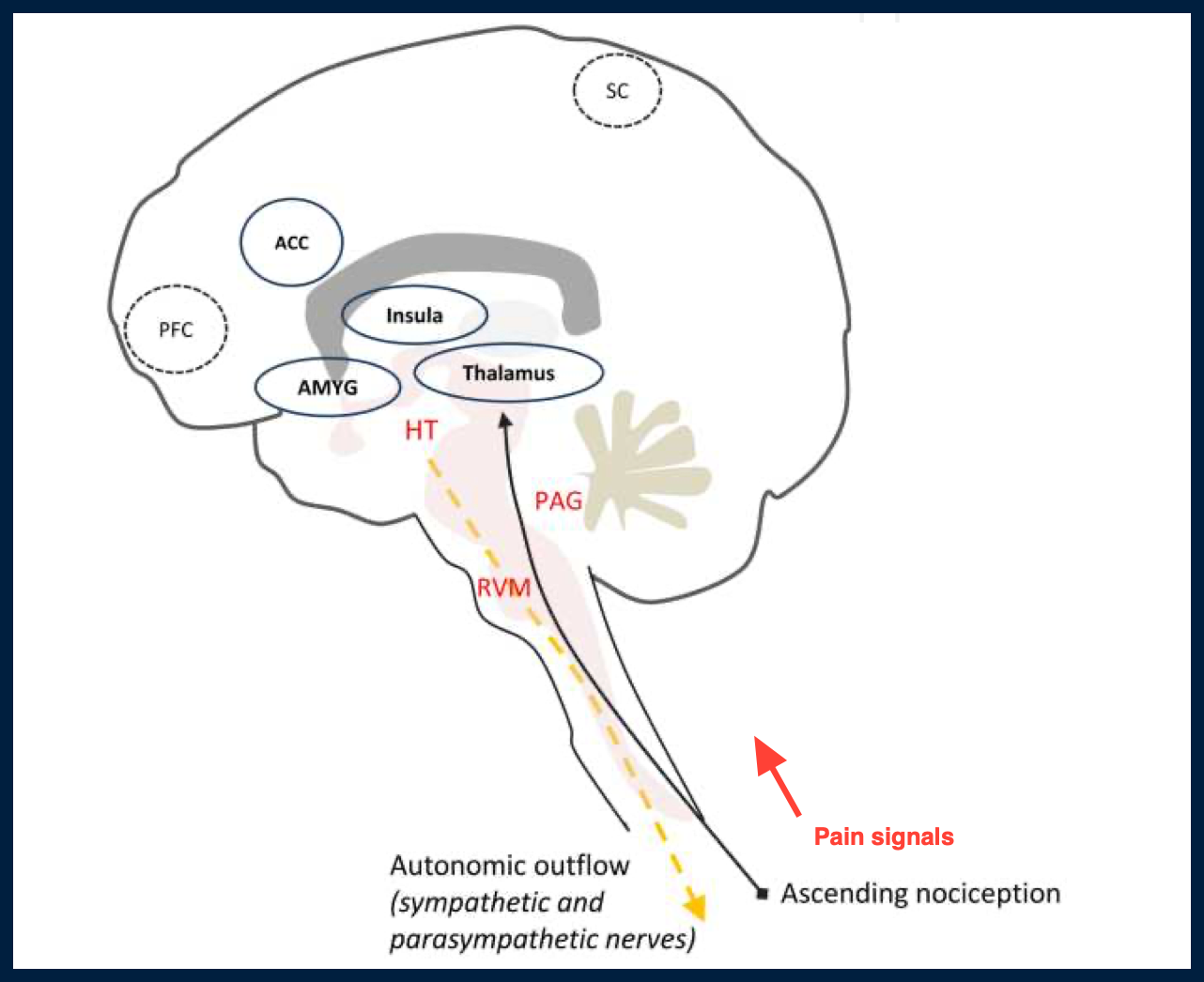
Here is where things start to get really interesting. Many of the areas in brain involved in ANS regulation are ALSO involved in pain regulation. The ANS and pain networks in the brain are deeply intertwined, reflecting a coordinated system that manages both pain and autonomic regulation. Like two mighty rivers that combine forces before dumping into the ocean, these brain systems together play a large role in fibromyalgia pain.
Key areas of brain involved in BOTH autonomic and pain processing include:
- Hypothalamus: crucial in regulating autonomic functions, and serves as one of the main regions for descending pain modulation. Captain of the SNS team
- Insula: pain processing,integrating bodily sensations (interoception), and controlling the ANS
- Periaqueductal gray matter: hub for integrating survival responses, defensive behaviors (fight/flight/freeze), and the perception/modulation of pain
- Parabrachial nuclei: plays a role in autonomic regulation, and receiving, processing, and relaying pain signals
- Locus coeruleus: involved in activating the fight-or-flight response, fear, autonomic responses, and pain modulation
The interactions between the autonomic nervous system (ANS) and pain perception go both ways. On the one hand, pain can affect how the ANS functions. On the other hand, alterations in autonomic arousal can also influence the experience of pain. Due to extensive functional overlap between structures involved in autonomic control and pain sensation at different levels of the spinal cord, brainstem, midbrain, and cortex, the ability of the ANS to modulate pain information is not surprising.
In the context of pain, a healthy ANS balance is key to managing the volume of pain signals. When the ANS is malfunctioning, the brain has less ability to properly regulate or block certain pain signals and pain volume spins out of control. The ANS and pain control networks are both broken in the fibromyalgia brain, and negatively impacting each other. It's a bit of a "chicken and egg" conundrum as to which came first. It's unclear how much altered ANS brain signaling results from altered pain processing, versus how much it is causing the pain processing problems.
Keep in mind that not every study of the shows abnormal ANS functioning in the brain in fibromyalgia. Some studies have shown conflicting results. For example one measured signal intensity in the locus coeruleus and found no difference between healthy controls and fibromyalgia brains. The story of the brain and fibromyalgia is complex and is an area of active research.
Connecting the dots
How does abnormal brain SNS activity fit into the big picture of what's happening in fibromyalgia? SNS hyperactivity is key to generating the fibromyalgia chain reaction, in my opinion. It's as if a switch is flipped on in the brain to push ANS to SNS mode, and gets stuck there. Because the SNS is involved in so many aspects of body functions, including immune function and pain regulation, this sets off a chain reaction that affects almost every system of the body and ultimately results in abnormal pain processing, central sensitization, nociplastic pain that is the most widely recognized problem in fibromyalgia. I view it as the end result of the chain reaction that starts in the SNS brain control network.
References and their primary conclusions
Studies indicate that the involvement of the autonomic nervous system at both the systemic and local levels is an important element of the pathogenesis of chronic musculoskeletal pain With chronic musculoskeletal pain, and also with chronic stress, the interaction between the nociceptive and autonomic systems appears to become maladapted.

FM group showed increased connectivity between the posterior cingulate cortex (PCC) and the thalamus, suggesting heightened saliency toward the noxious stimuli, which may contribute toward the mechanism which causes hyperalgesia in FM.
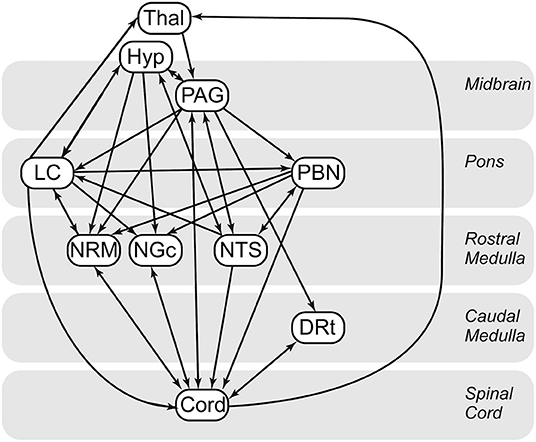
FM and control groups showed significant differences in brainstem/spinal cord network connectivity the LC, hypothalamus, PAG, and PBN, which are known to be associated with autonomic homeostatic regulation, including fight or flight responses. Altered pain processing in FM may be linked to changes in both descending pain regulation and autonomic regulation.
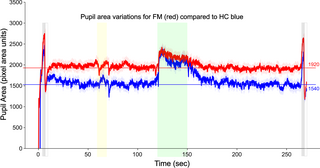
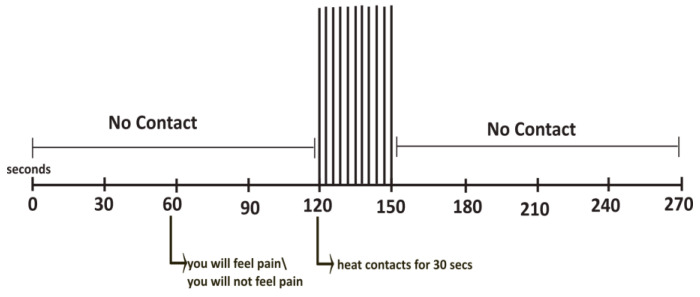
People with FM enter a heightened state of neural activity associated with anxiety and autonomic functioning concurrent with increased pupil sizes, and heightened pain sensitivity. These findings may relate to the well-known hypervigilance and global hypersensitivity of FM participants.
Results provide new evidence of altered neural signaling in FM related to arousal and autonomic homeostatic regulation.
Findings link cardiovascular autonomic parameters to brain activity changes involved in the elaboration of nociceptive information, thus beginning to elucidate underlying brain mechanisms associated with the reciprocal relationship between autonomic and pain-related systems.
LC signal intensity did not distinguish participants with fibromyalgia and healthy controls, nor was it associated with core fibromyalgia pain symptoms. Dynamic measures of noradrenergic function may be required to understand noradrenergic contributions to fibromyalgia.