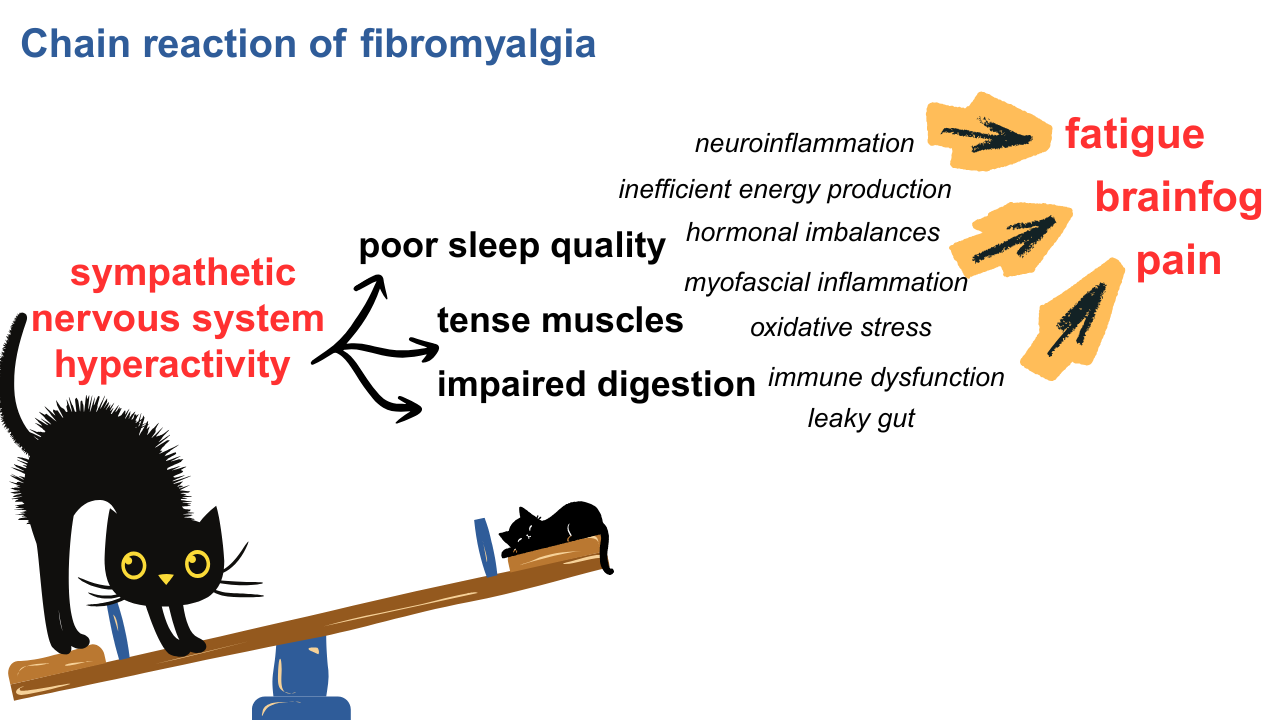
The sympathetic nervous system (SNS) is hyperactive in fibromyalgia. In my opinion this abnormality causes a chain reaction that leads to all of the symptoms of fibromyalgia. But my chain reaction theory is just that, a theory and it is the way I personally connect the dots. So it is a subjective way of looking at the big picture of fibromyalgia. But the dots themselves, the individual data points gathered by scientific studies, are objective and do not rely on my opinion.
This post gives an overview of the SNS, the different ways it can be studied and what each method reveals about sympathetic hyperactivity or dominance in fibromyalgia. First, let's start with the basics.
What is the Sympathetic Nervous System?
The SNS is one branch of the Autonomic Nervous System (ANS), which is the “autopilot” that controls most basic housekeeping functions of the body, like blood pressure, heart rate, breathing, digestion, sleep and urination. It consist of two different sets of nerves that have opposing functions. For example, one set of nerves constricts blood vessels while the other dilates blood vessels.
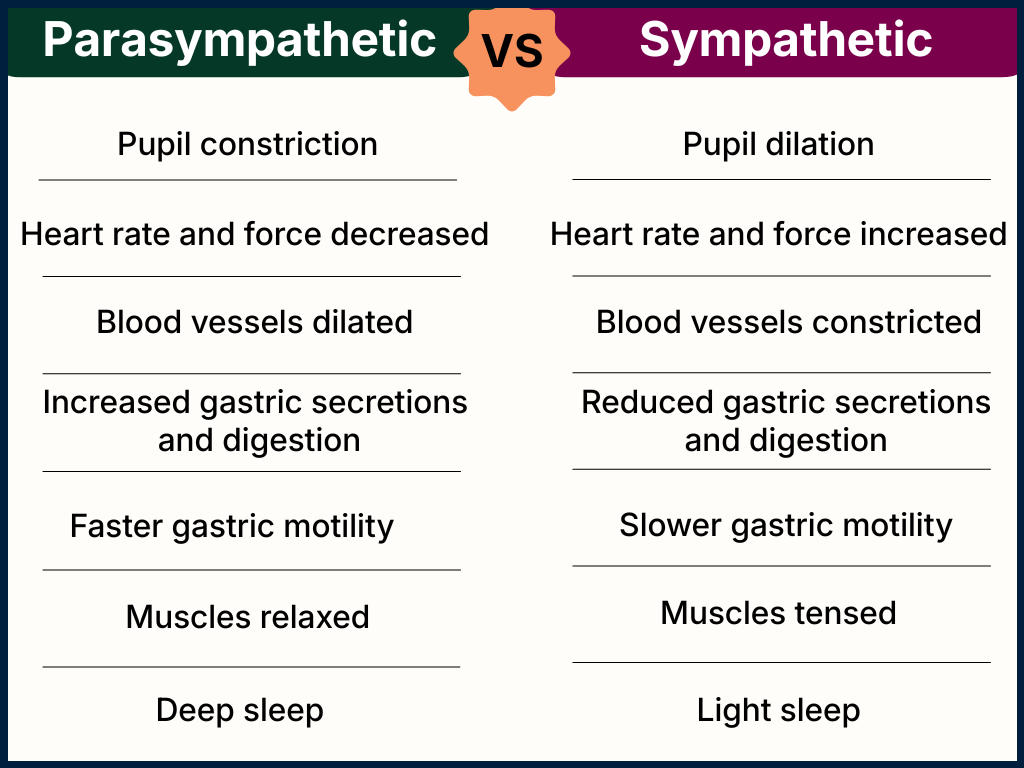
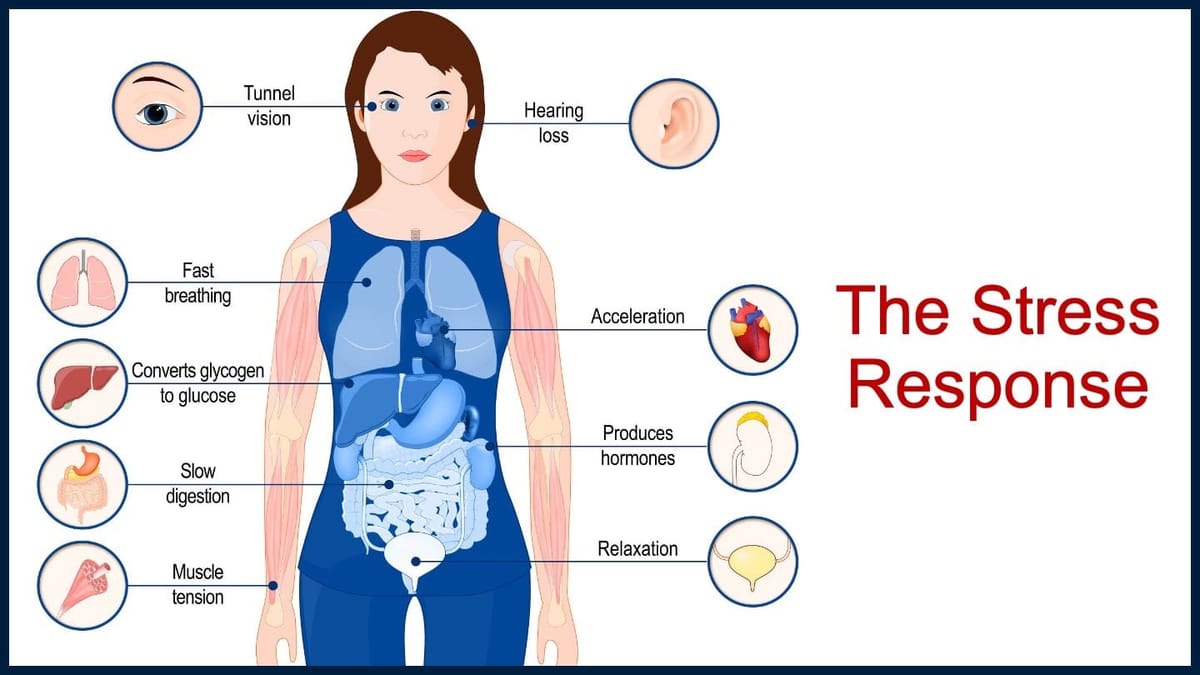
One nerve network consists of the sympathetic nerves which are often compared to the accelerator in a car. Actions of the SNS prepare the body to respond to a threat by tensing the muscles, dilating the pupils, and increasing the heart rate in what is known as the fight-or-flight response. The opposing network is the parasympathetic system (PNS) and this is often compared to the brakes of a car. Actions of the PNS prepare the body for rest, by relaxing muscles, slowing the heart rate, increasing digestion in what is called the rest-and-digest response.
When functioning normally the ANS is constantly shifting the balance between these contrary responses, just like when you drive a car, you modulate the gas pedal and brake to control your speed. The ANS causes very subtle and brief shifts in the body that keep things running smoothly. For example, the action of standing up would cause a big drop in your blood pressure without the brief activation of sympathetic nerves to constrict blood vessels in your legs. But in fibromyalgia, the balance is off, and is skewed towards SNS activity all the time. Imagine all the problems you might run into trying to drive a car that has a powerful gas pedal and a weak brake pedal.
If the car analogy isn't working for you, think of the SNS and PNS as two sides of a see-saw. Each side moving up and down as needed to adjust to body's needs. But what if the cat sitting on the SNS side of the seesaw is really heavy? The seesaw is going to get stuck in that direction. That is the SNS dominance we see in fibromyalgia and it has wide-ranging negative actions all over the body.
Summed up perfectly by one of my favorite scientists who often uses delightfully colorful language in his articles (a refreshing change from typical dry and bland scientific writing!). Dr. Martinez-Lavin has been writing about and studying "relentless sympathetic hyperactivity" in fibromyalgia for over 25 years.
The SNS is hard to study
The balance of the ANS is difficult to evaluate in clinical practice because it is constantly shifting. Changes in breathing pattern, presence of mental stress, or even change in posture can dramatically alter the sympathetic and parasympathetic balance. In the same way your usage of gas pedal and brake is constantly shifting while driving as you respond to different road conditions and traffic. There are some scientific ways to measure the position of the ANS seesaw and determine the ratio of PNS to SNS (brake to accelerator usage). However the autonomic nervous system is notoriously difficult to study because it is constantly fluctuating, moving and shifting as it balances hundreds of bodily functions happening all at once. It's a bit like trying to diagnose engine trouble on the freeway by climbing on the front of the car, popping the hood and watching the engine parts move as you drive 70 miles per hour.
So scientists studying the moving target of the ANS instead have to take snapshots of different parts of the engine, and try to piece the picture together. This is complex and challenging to accomplish. Activity of the sympathetic nervous system can be measured in a variety of ways, but no method is perfect.
Although there is loads of science showing SNS in hyperdrive in FM, it has not been widely accepted as a definitive source of FM symptoms. However part of why I feel so confident that SNS problems play a huge role in fibromyalgia is because I have the inside scoop, so to speak. I am studying fibromyalgia from the inside, and I can FEEL in my fibro body, how my muscles are clenched, how hard it is to fall asleep, how my GI system and urinary systems are malfunctioning. Often when I describe the hyperactive SNS in fibromyalgia it really resonates with others living with the illness and I hear things like "That's exactly what it feels like is happening in my body!" Of course intuition and anecdotal experience have only limited value from a scientific perspective, but they do have some value. They can provide useful directional guideposts to show us where to look and give context to what we see in studies.
SNS activity in fibromyalgia
I am not the only one who has noticed the sympathetic nervous system dominance in fibromyalgia. Here are some other ways I have seen it described by various scientists and researchers:
“riotous activation of this system in FM”
“rigid sympathetic hyperactivity”
“relentless sympathetic hyperactivity”
“a deranged sympathetic response”
"unrelenting sympathetic hyperactivity throughout the day, associated with a deranged sympathetic response to different stressors. "
"sympathetic nervous system that is persistently hyperactive but is hyporeactive to stress"
"malfunction of the sympathetic component of the stress response system".
How have they come to these conclusions? Although it is difficult to study the ANS, it is not impossible.
Seven different ways to measure SNS activity
- heart rate variability
- tilt table test
- sympathetic skin response
- muscle sympathetic nerve electrical activity
- symptom surveys
- brain activity in areas controlling ANS
- blood levels of epinephrine and norepinephrine
Below is a brief video overview of each of these techniques and what they show in fibromyalgia, followed by written explanations. Some topics are explored in more detail in separate posts.
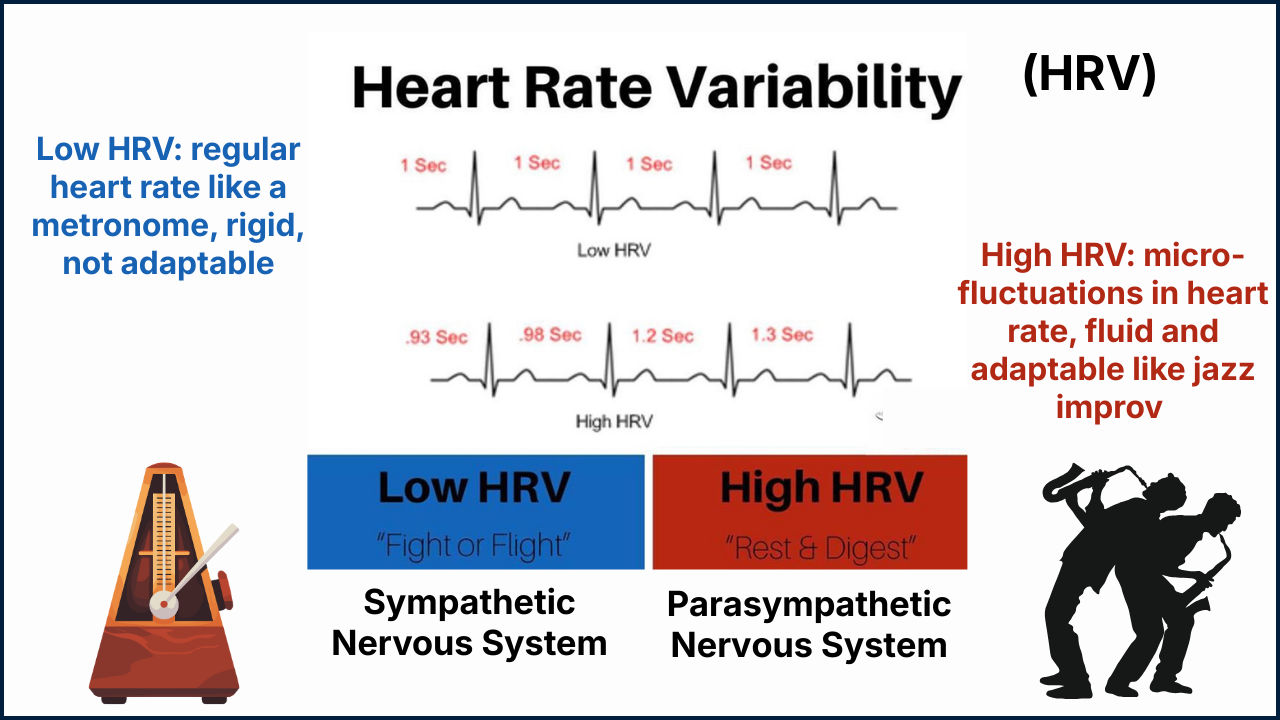
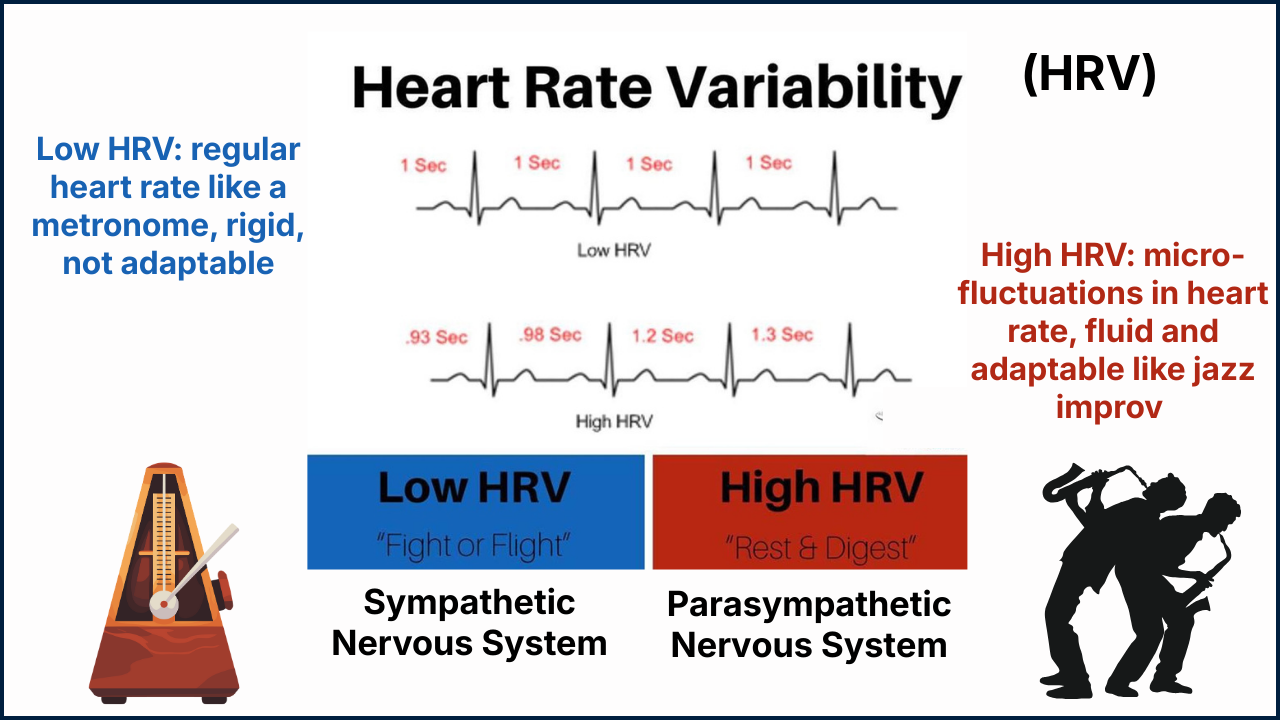
Heart Rate Variability (HRV)
Heart rate variability refers to the natural beat-to-beat changes in your heart rate and reflects the balance between the sympathetic and parasympathetic nervous system. We see low HRV when the SNS is dominant and high HRV when the parasympathetic nervous system is dominant.
At least 14 separate studies have found HRV to be reduced in FM, reflecting sympathetic dominance. And two different systematic review articles reached same conclusion, with one writing:
“From the literature review, a clear pattern of sympathetic abnormalities in FM emerges: basal sympathetic hyper-activity accompanied by blunted sympathetic response to different types of stressors. HRV alterations suggestive of sympathetic dysfunction are perhaps the most consistent alteration described so far in FM.” Martinez-Lavin 2011
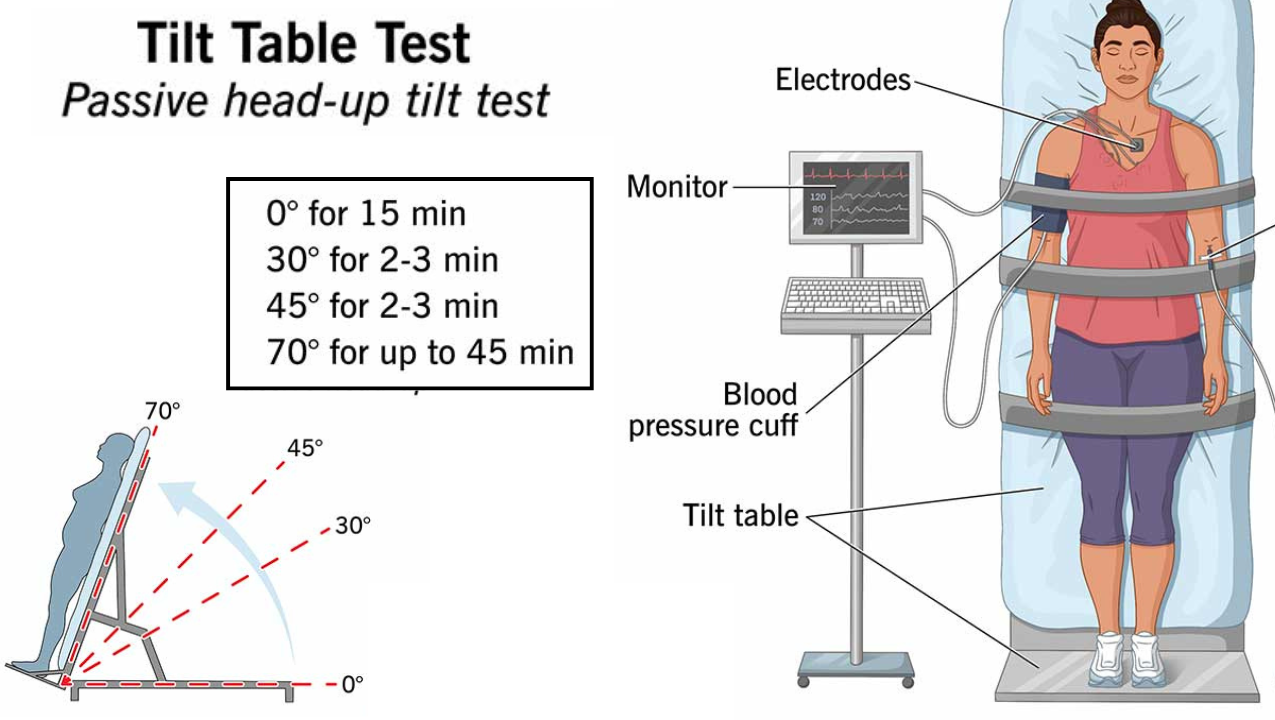
Tilt table testing
Another way to measure sympathetic activation in the body is by seeing how well the body can respond to position changes like standing up, as this response is dictated by the autonomic nervous system. Tilt-table testing creates passive changes in posture that allows for targeted measurements of the SNS response to changes in body position changes, which in fibromyalgia is not very well at all!
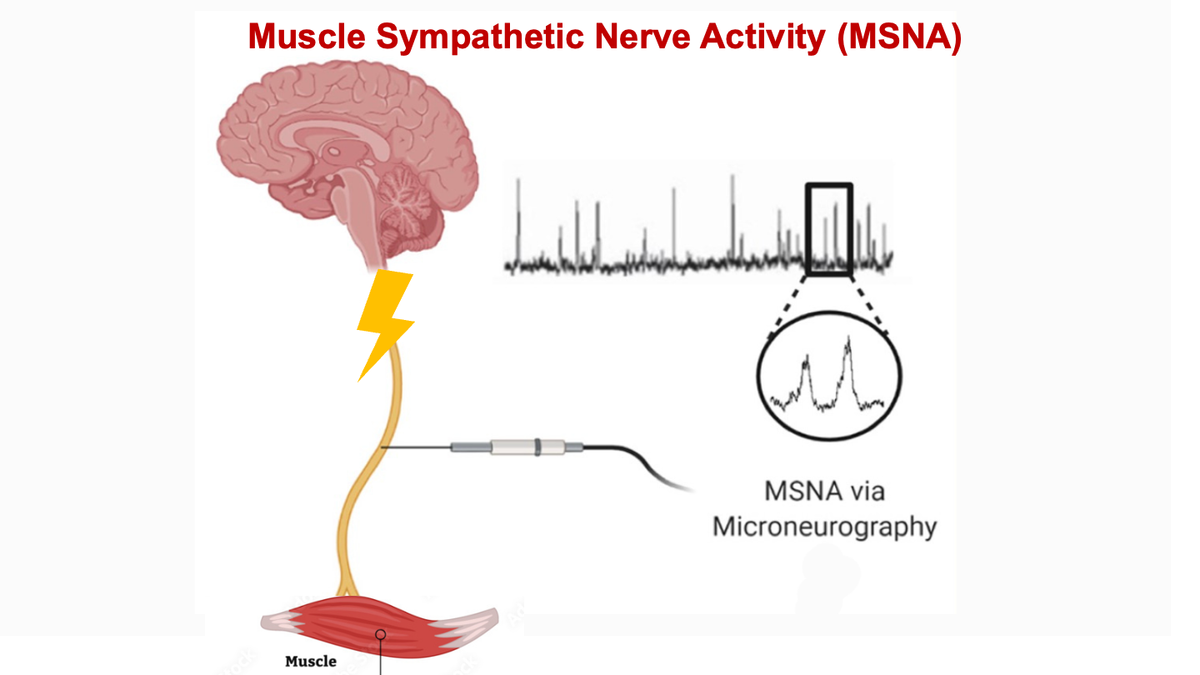
Muscle Sympathetic Nerve Activity (MSNA)
We can also measure how much electrical activity the brain is sending down the sympathetic nerves to our body, in particular to the muscles. This electrical activity is measured in pulses or bursts, a higher burst rate reflects more SNS messages coming down from the brain. MSNA elevated in fibromyalgia almost to the ceiling level, and is therefore not able to increase much when the body needs electrical activity to increase. And that is why we tend to fail the tilt-table test.
Sympathetic Skin Response
Sympathetic relay stations near the spinal cord sends electrical signals all over the body, and some head to the skin to regulate sweating. Triggering and then measuring these electrical signals to the skin gives us a way to measure SNS activity, called the Sympathetic Skin Response (SSR). It's an indirect, but still useful, way to measure the volume level of the SNS system, which is turned yup very loud in fibromyalgia.

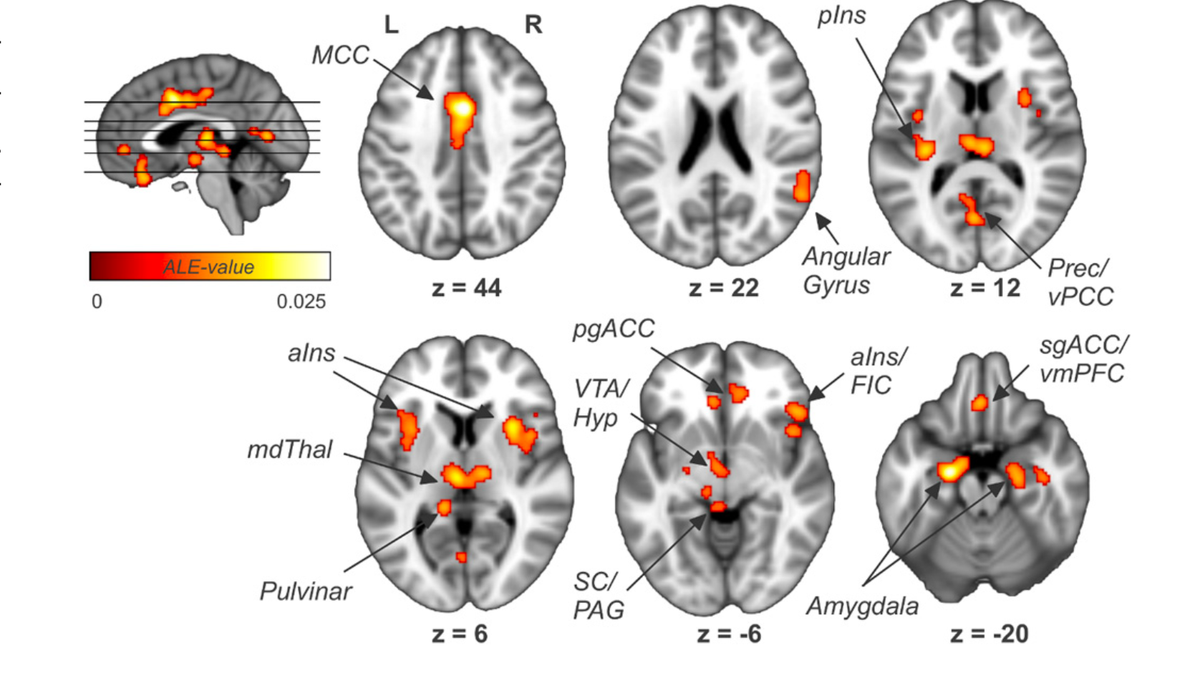
Brain Evidence
Imaging studies demonstrate abnormal levels of function in brain regions that control the ANS. There also abnormally strong connections in the brain between the different regions that regulate the ANS. The brain regions responsible for autonomic control and pain perception are very close together and interact extensively. So any ANS alteration can affect how our brain processes pain signals, leading to the central nervous system amplification of those signals.
Symptom Surveys
The Composite Autonomic Symptom Score (COMPASS-31) is a standardized tool for assessing autonomic dysfunction based on patient rating of presence and severity of symptoms. Several studies have shown that women with fibromyalgia scored much higher on the COMPASS-31 questionnaire compared to healthy controls. This survey is particularly useful to evaluate fibromyalgia symptoms that are not pain-related such as sleep disturbances, fatigue and orthostatic intolerance.

Blood levels of epinephrine and norepinephrine
In response to stress, the hypothalamus signals directly to the adrenal glands via the sympathetic nerves and tells them to make more epinephrine (also known as adrenaline) and norepinephrine (also known as noradrenaline). These chemicals help enact the fight-or-flight response. Norepinephrine has more focused effects and also has an important role as a neurotransmitter. Epinephrine has more wide-ranging effects and relies mostly on hormonal actions. If we are dealing with SNS hyperactivity in fibromyalgia would expect to see elevated levels of these chemicals. Which we do...sort of.
Results have been inconsistent with some studies showing elevated levels and some finding normal levels. Partly this may be due to difference in study settings and methods, because levels of epinephrine and norepinephrine are constantly fluctuating. A 2023 meta-analysis (a review that lumps related studies together to try to get at the 'big picture' of what the data is saying), reported overall norepinephrine levels are higher in FM, although no difference was seen in epinephrine levels.
Although this post ends with a whimper rather than a bang, some of the other data supporting SNS hyperactivity in FM is much more definitive, with the loudest signal coming from heart rate variability, so let's go there first!